What is OASI?
The Obstetric Anal Sphincter Injuries (OASI) Bundle is a group of interventions which aims to reduce the number of injuries up to and into the anal sphincter which can happen during a vaginal birth.
It was created in an attempt to reduce the average rate of OASI in the UK, which at the start of the trial stood at around 3.3%, or 33 in every 1000 women, according to RCOG(1) . RCOG estimates that from 2017 to the end of the trial, it has been reduced by 0.3%, to 30 in every 1,000 women, by the use of the OASI Bundle (1) , although the final results are not yet available.

The interventions are:
1 ) Inform the pregnant woman or person about the risk of OASI, and what can be done. This should be done before labour starts, and is intended to be a discussion of the risks and benefits of the OASI bundle, in order to obtain full informed consent. It is unclear whether the bundle includes the request to also discuss the risks and benefits of other options which may reduce OASI, although this would be legally required as part of the consent process for the procedure.
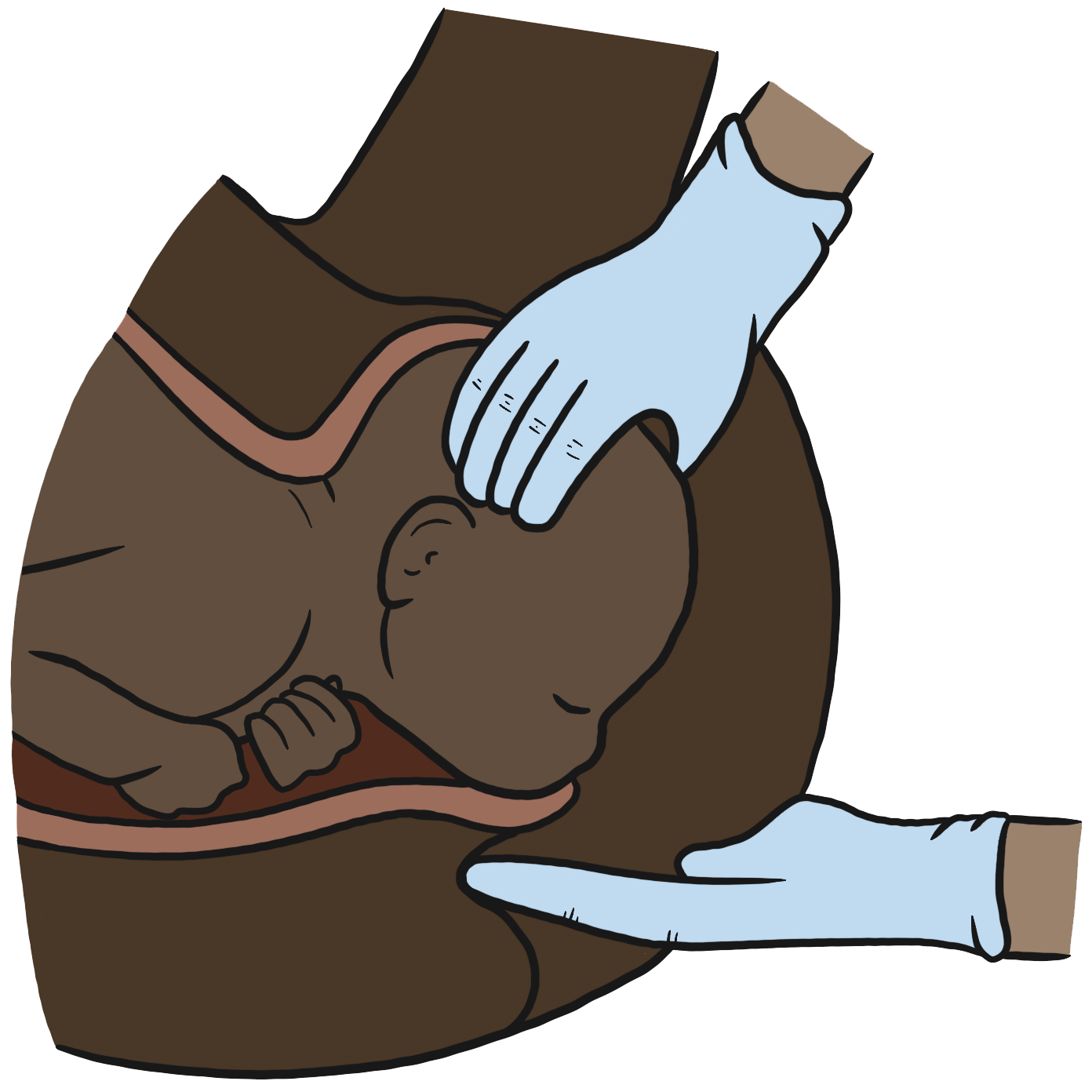
2 ) Assuming that the pregnant woman or person gives their consent (and doesn’t remove their consent at any time), the midwife or doctor will use their hands to support both the perineum and the baby at the point of birth, while directing the woman’s pushing to try to slow the birth of the head.
3) Use of episiotomy is part of the bundle, “only when essential”. There is some explanation of what “essential” means in the FAQ (1) although consent is not mentioned in the explanation.
4 ) After birth, the midwife or doctor should offer to check the woman or person’s vagina, perineum and rectum for tears.
There is absolutely no doubt that an obstetric anal sphincter injury can be a life changing injury. Many women and people have felt too embarrassed to seek medical help, and for those who do, reconstructive surgery can lead to more physical and mental trauma, and it is not always successful.
If a clinician doesn’t spot an OASI after birth this could lead to a claim of negligence. It can also make repair harder, if some healing has happened, for instance if the woman or person seeks support some months (or longer) down the line. The extra costs to the NHS of resolving these issues are mentioned as part of the reason for trialing the OASI Bundle.

When trials aimed at reducing poor birth outcomes are critically analysed, there is sometimes a perception that if there is criticism of the trial that the criticism is aimed at the intention of the trial (in this case, to reduce serious tears and also to spot tears which might previously have been missed). It is very important to recognise that this is not the case.
All of us are on the same team: OASI is a most unpleasant birth outcome and everyone wants to see it reduced. However, it is absolutely appropriate to evaluate whether or not the OASI Bundle is the best way to reduce serious tears, whether there might be alternatives, and whether there might be problems with the Bundle that the researchers may not be recognising.
There are a number of issues around the OASI bundle which we want to explore:
- Rates of OASI and birth location
- Tears through the clitoris (anterior tears)
- Information sharing and consent

Rates of OASI, birth location and birth position.
Before the OASI Bundle was rolled out, nearly one in
thirty women and people who give birth vaginally in
the UK experienced a tear which reached or included the anal sphincter. That means that nearly one in every thirty people who gives birth in the UK may have what can be a life changing injury (1). These statistics are horrifying. How can it be that so many women are experiencing this injury?
Birthing outside of hospital leads to a much lower rate of third and fourth degree tears.
Studies which looked at the rates of serious tears at home compared to hospital birth found rates as much as 5 times higher in the hospital (2) . In the UK, The Birthplace Study showed that just planning a home birth (even if the woman ended up birthing in hospital) led to a 1.9% rate of third and fourth degree tears compared to 3.2% in hospital or alongside maternity units (2) .
Information gathered from a self-reporting survey of 54 homebirth midwives showed the following:
| % 3rd degree | % 4th degree | |
| Independent Midwives | Less than 0.5% | 0% |
| NHS Midwives | Less than 1% | 0.08% |
Why doesn’t the OASI Bundle look at birth location as part of its attempts to reduce the high rates in UK hospitals? And furthermore, why is there such a difference between home and hospital?
Perhaps one reason may be that where birthing women and people are more relaxed, they are more likely to have a more relaxed perineum.
Strangers looking at our vulvas will make any of us feel exposed and uncomfortable. When we go for examinations such as a smear test we are reminded to relax… relax… and many of us will remember how allowing tension to flow from our bodies makes the speculum feel less uncomfortable. And yet, at the point that a baby is about to be born, what happens far more often than it should? A midwife takes a torch out and takes a look. Sometimes a doctor comes into the room, and even if they properly introduce themselves and ask for permission to look at the woman’s vulva, they are another pair of eyes on her. Suddenly, we are exposed and vulnerable. We may pass stool – maybe the first time in our adult life that this happens in front of others. We are in a clinical environment, where we are unlikely to have built a relationship with our midwife or doctor. Is it any surprise that we might feel like tensing up?
But there is another reason….the physiology…
The Real Birth Programme helps understanding of the changes that are taking place within the area of the perineum as birth progresses.
The perineum is a complex and perfectly designed group of muscles that thin out and stretch to assist the passage of baby. Growth of the muscle and the skin of the perineum is aided by the hormones released in pregnancy. Then, as the baby’s head or bottom is passing by the rectum a hormonal feedback response is triggered that keeps the muscles of the perineum relaxed.
At the same time, the muscles of the perineum produce a counter pressure on the presenting part of the baby. In most births this is the area surrounding the occiput. This counter pressure creates moulding of the head and this moulding ensures that the baby’s head can reduce to the smallest diameter to carry on its journey through the birth canal with ease.
All the while, a continuous feedback response is created that helps to keep the muscles of the perineum soft. The muscles are really vascular, meaning that they have a high number of blood vessels feeding them. Within the flow of blood contains the hormones that keep the muscles soft.
The pressure from the uterus, through baby’s pole or core , gently stretches these muscles. Whilst there is a blood flow to the perineum this process happens more quickly and with less stress and trauma on the muscles. The flowing blood acts as a ‘cushion’.
We believe that directed pushing and lying on your back with your legs wide open causes this natural feedback loop to be broken. The reduction of oxygen and blood flow through directed pushing, which involves breath holding and forced sustained pushing, creates additional resistance within these muscles.
The resistance comes from forcing the presenting part (normally baby’s head!) onto the muscles. This additional sustained pressure depletes the blood flow for longer that it would naturally be reduced for, which increases the resistance in the muscles, making the muscle fibres less flexible and more at risk of tearing. The reduced blood flow also reduces the levels of hormones that are there to assist with the flexibility and growth of the perineum.
If we look at athletics it is well understood that muscles that are depleted of oxygen for longer periods of time result in cramps, tearing and damage.
Add this now to the position of being on your back.
Having your legs wide open places additional pressure on the perineum, additional pressure, where there is a counter pressure in the opposite direction also occurring simultaneously from the uterus through baby. This places more pressure on the baby’s head than is biologically normal.
More pressure on the baby’s head leads to higher pressure on baroreceptors within the already moulding head, creating greater changes in the heart rate as the baby tries to conserve oxygen by slowing the heart rate down even more, leading to the birth attendants to ask the woman to push harder. It is these practices that can contribute to OASI.
People birth in tights, pants, and trousers, without their legs wide open and very rarely are there tears. The instinct to close our legs is there, so we close our legs and help protect the perineum.
The natural instinct to close the legs at birth also opens up the pelvic outlet as the baby’s shoulders pass through it ready for birth, making room for the shoulders through the boney structures.
It is so easy, as a midwife, obstetrician or other birth worker, to forget that while we might have seen many, many vulvas, the person in front of you has never had you looking at their vulva. That really matters to them. The mantra “leave your dignity at the door” no longer applies in birth (and never should have).
Continuity of carer, that is, having a known and trusted midwife through pregnancy, labour and beyond, would make a huge difference to the ability of birthing women and people to relax and listen to their own bodies at this critical point in their labour. As would birth attendants remembering to treat all birthing people’s genitals with the same dignity that they’d like to experience themselves.

Another possible reason that birth outside hospital leads to much lower rates of OASI is birth position.
While, in theory, birthing women and people in hospital are free to move into any position they wish, in practice the fact that the bed is central to the room means that most people just ‘hop up on the bed’ and, when in bed, we lie down.
Unless women and people are discouraged from doing this it is the most likely position they will labour and birth in. Many women also report being asked to lie down, or to get into a semi-recumbent position for birth, even if they’ve been active in other positions during the earlier part of their labour. In our recent survey on birthing positions, a overwhelming majority are asked and encouraged by their midwife to lie down.
Women can be often be asked to open their legs, and sometimes their legs are held open (which is illegal assault), yet when supported to follow their own instincts they often close their legs at the point that the baby is about to crown. Overriding a woman’s instincts, which are driven by sensations that only she can feel, should be over-ridden by the birth attendant at their peril. Or, rather, at the peril of the woman’s perineum.
Birth positions can be hugely influential on the chances of a serious tear. Upright (including standing,) forward leaning and all-fours positions are positions which lead to the lowest chance of injury. Squatting and semi-recumbent and lithotomy the most likely positions to lead to perineal injury (4.5). Women are more likely to be off the bed and off their back if they are not in the hospital.
Despite this, many midwives report that they are encouraged to ask the woman or person in their care to actually move into a semi-recumbent position as birth approaches, even if they were labouring in a better position to avoid OASI, so that the ‘hands on’ part of the bundle can be done. In other words, women are being asked to go into a more risky position in order that the Bundle can be used to try to reduce their risk.
While the ‘hands on’ technique is supposed to be able to be used in multiple positions, many midwives who shared their experience said that they were not adequately trained to do it in another position other than semi-recumbent. One midwife reported, “I cannot get training to do this in any other way, yet woe betide me if I don’t do it, so I have no choice but to ask them to get onto the bed.”
The OASI Bundle information pages, include a video which shows a model of an abdomen, vulva, thighs and a crowning baby. This model reduces women to their birthing parts, and does nothing to remind birth attendants that they have a responsibility to the whole person, not just their genitals. The model shows someone on their back, with their legs in an uncomfortably pulled back position. If you try to get your legs into this position you will find it may impact your breathing! It would be difficult to balance the model to show a side-lying or all fours position. With this being the training shown on the promotional video (1) for the OASI Bundle, it is not a surprise that so many are struggling to understand how to support the perineum in any other way than with the woman in a semi-recumbent position.
Understanding the physiology is key…
Tears through the clitoris.
One concern about the OASI Bundle is whether it could lead to higher numbers of anterior tears – tears towards the front of the body – as the pressure is redirected away from the posterior side of the vulva.
The OASI Bundle FAQ states, “anterior tears are usually more straightforward to repair than a third or fourth degree tear and do not have severe long term effects on the woman.” (6)
And yet, this is not the experience that women report.
Anterior perineal injuries can cut through the clitoris, causing long term loss of sexual sensations. The clitoris is a large structure, far greater than the small nub which can be easily seen and felt. It has two ‘legs’ which hug the vagina and urethra, and so any anterior tear can lead to injury to this essential organ. It is concerning that there is no recognition that a loss of sexual sensation are “severe long term effects”. The document says that data on anterior tears, including those into the urethra, will be collected, but at the time of writing RCOG was unable to provide this data
Information sharing and Consent.
Midwives and doctors need to be extremely confident that they have obtained absolutely clear informed consent from the woman or person in their care before gripping a birthing woman or person’s perineum. This is essential in order to avoid the risk of an accusation of criminal assault.
Touching anyone’s genitals can only be done with their consent. Consent for a routine intervention must not be gained at the point of crowning because this does not give the woman or person time to make an informed decision.
It is imperative, legally, morally and ethically, that a full
and frank conversation happens with everyone who is
pregnant.
The conversation needs to include:
The reason why the OASI Bundle is being offered – and that it is an offer which can be accepted or declined.
An explanation of the fact that it is a type of trial – data is being collected to see whether the Bundle does, or does not, lower the chance of obstetric anal sphincter injury
An explanation of the possible risks including pain, trauma and a possible increased risk of anterior tears and their consequences
An explanation of alternatives which may reduce the chance of a severe tear. For example, non-directed pushing, warm compresses (6) , trusted caregivers and a calm environment to minimise
The very first element of the four elements of the OASI Bundle is the instruction to explain what OASI is, and what can be done to reduce the chance of it happening. This cannot simply mean talking about the OASI Bundle intervention and it cannot happen during birth. While informed consent can be given for interventions that were not planned before birth, absorbing enough information to make a decision is harder when in labour. The OASI Bundle is a planned intervention which therefore has to happen before birth.
Without informed consent, the intervention is criminal assault.
If you are a midwife or doctor who is reflecting on their offering of the OASI Bundle, can you honestly say that:
You are fully explaining the benefits, risks and alternatives without trying to encourage the woman or person to accept the OASI Intervention?
You are only doing this before labour starts and documenting the woman or person’s decision?
You are confident in performing the hands-on element of the OASI Bundle with the woman or person in all possible positions? You don’t encourage her onto her back for your convenience or because of a lack of training on any alternative position?
If you are driving the implementation of the OASI Bundle, are you ensuring that your staff are protected from accusations of criminal assault, and the women and people in your care are protected from assault by ensuring that staff have the time to discuss OASI properly?
In conclusion, the data that the OASI Bundle collects may be extremely informative, and may be part of an important change which leads to a reduction in the chances of serious obstetric tears. However, there are serious questions which must be addressed about consent and information sharing, as well as questions which must be answered about why other aspects of care are not being considered as a solution. Given the much lower numbers of OASI that happen at homebirths and with known and trusted care givers, it is time for obstetricians, midwives, and the Bundle creators to reflect on whether conventional childbirth hospital practices are the cause of many of the injuries that they are trying to resolve.
References
- OASI Bundle overview published by RCOG: https://www.rcog.org.uk/OASICareBundle
- Birthplace 2011, table 29: http://www.netscc.ac.uk/hsdr/files/project/SDO_FR4_08-1604- 140_V03.pdf
- Meta-analysis of the Safety of Home Birth: https://pubmed.ncbi.nlm.nih.gov/9271961
- Risk Factors for Anal Sphincter Tears: The Importance of Maternal Position at Birth: https:// pubmed.ncbi.nlm.nih.gov/17877679/
- Birth position and obstetric anal sphincter injury: a population-based study of 113 000 spontaneous births: https://bmcpregnancychildbirth.biomedcentral.com/articles/10.1186/s12884-015-0689-7
- OASI FAQ published by RCOG: https://www.rcog.org.uk/en/guidelines-research-services/audit-qualityimprovement/oasi-care-bundle/oasi-faqs/
- WHO recommendation on techniques for preventing perineal trauma during labour: https:// extranet.who.int/rhl/topics/preconception-pregnancy-childbirth-and-postpartum-care/care-duringchildbirth/care-during-labour-2nd-stage/who-recommendation-techniques-preventing-perinealtrauma-during-labour
- Fear causes tears – Perineal injuries in home birth settings. A Swedish interview study: https:// www.ncbi.nlm.nih.gov/pmc/articles/PMC3034711/#B13




{kind=link}